

𝟏𝟎 Rules of A Normal ECG
Rule 1: PR Interval
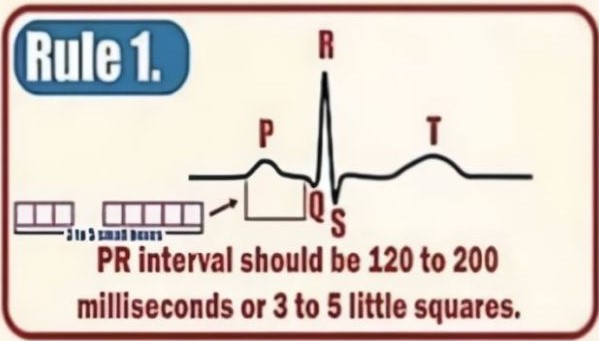
- Definition: The PR interval represents the time from the onset of atrial depolarization (P wave) to the onset of ventricular depolarization (QRS complex).
- Normal Range: 120–200 milliseconds (ms) or 3–5 small squares on ECG paper.
- Clinical Importance:
- A prolonged PR interval (>200 ms) suggests first-degree AV block.
- A short PR interval (<120 ms) may indicate pre-excitation syndromes like Wolff-Parkinson-White (WPW) syndrome.
Rule 2: QRS Complex Width
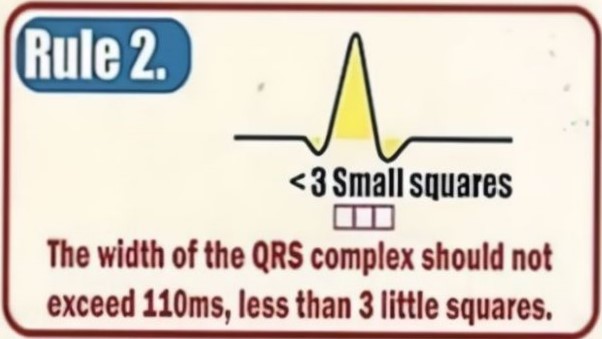
- Definition: The QRS complex represents ventricular depolarization.
- Normal Width: Should not exceed 120 ms (or less than 3 small squares).
- Clinical Importance:
- A wide QRS (>/=120 ms) may indicate bundle branch block, ventricular tachycardia, or hyperkalemia.
Rule 3: QRS Complex in Leads I and II
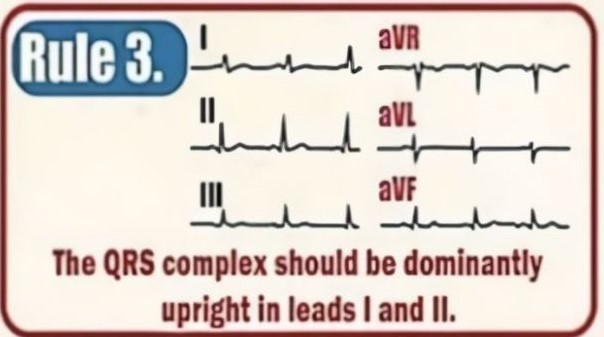
- Observation:
- The QRS complex should be predominantly upright (positive deflection) in leads I and II.
- Clinical Importance:
- If QRS is negative in these leads, it may indicate axis deviation, chamber enlargement, or conduction abnormalities.
Rule 4: QRS and T Wave Direction
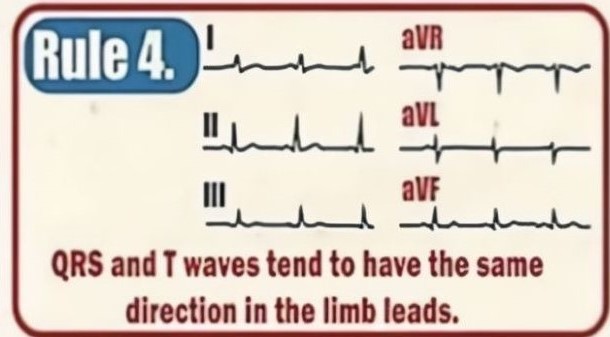
- Observation:
- QRS and T waves should typically be in the same direction in limb leads.
- Clinical Importance:
- If T wave is opposite to QRS, it may suggest ischemia, electrolyte imbalance, or repolarization abnormalities.
Rule 5: aVR Lead
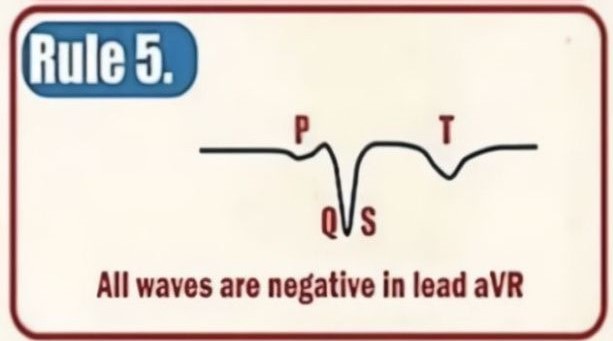
- Observation:
- All waves (P, QRS, and T) should be negative in lead aVR.
- Clinical Importance:
- If the waves are positive, it suggests incorrect lead placement or a rare condition affecting ventricular activation.
Rule 6: R and S Wave Progression in Precordial Leads
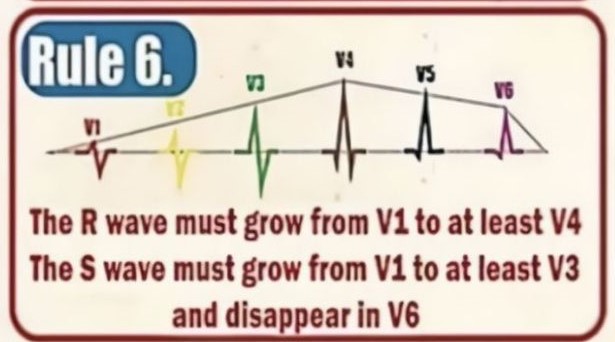
- Observation:
- The R wave should progressively increase from V1 to V4.
- The S wave should progressively decrease from V1 to V3 and disappear in V6.
- Clinical Importance:
- Poor R wave progression may indicate old anterior myocardial infarction or left ventricular hypertrophy.
Rule 7: ST Segment
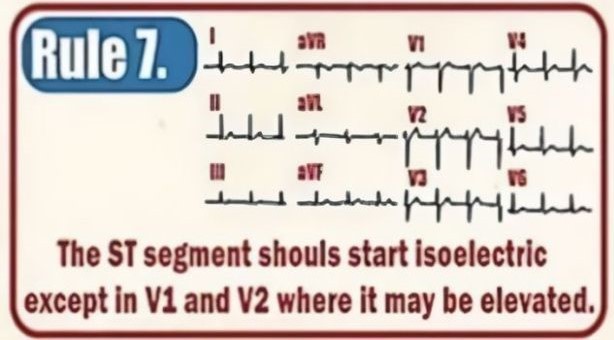
- Observation:
- The ST segment should be isoelectric (flat), except in V1 and V2, where it may be slightly elevated.
- Clinical Importance:
- ST elevation may indicate acute myocardial infarction (STEMI).
- ST depression suggests ischemia or electrolyte imbalances.
Rule 8: P Wave Morphology
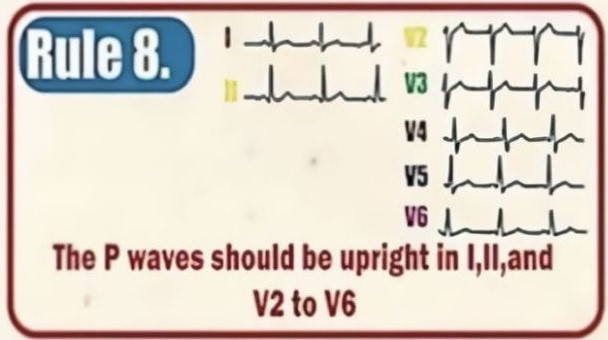
- Observation:
- The P wave should be upright in leads I, II, and V2 to V6.
- Clinical Importance:
- Inverted P waves in these leads may indicate ectopic atrial rhythms.
Rule 9: Q Wave Characteristics
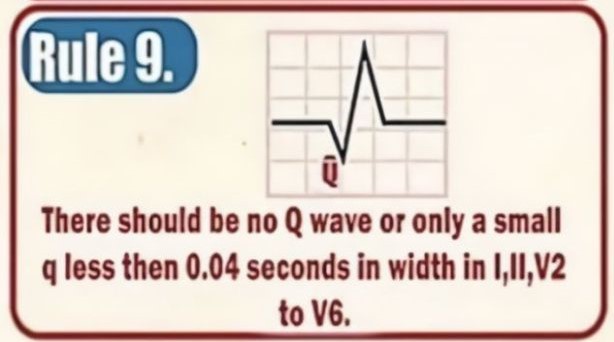
- Observation:
- There should be no pathological Q wave, or only a small q wave (<0.04 seconds) in leads I, II, V2-V6.
- Clinical Importance:
- Deep Q waves (>0.04s and >25% of R wave height) may suggest previous myocardial infarction.
Rule 10: T Wave Morphology
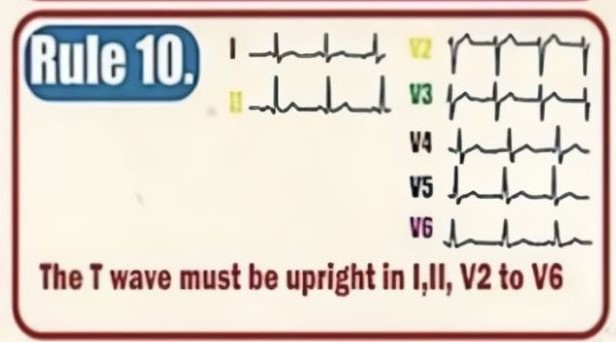
- Observation:
- The T wave must be upright in leads I, II, V2 to V6.
- Clinical Importance:
- Inverted T waves may indicate ischemia, strain patterns, or electrolyte abnormalities.
Do not forget to leave a comment, if this helped you in anyways… THANK YOU !!!
